Random Patient Generator

Dr John Wilkinson is a clinical teaching fellow in Anaesthesia and Intensive Care Medicine at the Freeman Hospital, Newcastle upon Tyne.

Dr Sarah Redford is a Primary Care Physician, Training Programme Director and Lecturer at Newcastle University.

Janet Wilkinson is an Advanced Critical Care Practitioner working at the Freeman Hospital, Newcastle upon Tyne.

Dr Matthew Faulds is a Consultant in Anaesthesia and Intensive Care Medicine at the Freeman Hospital, Newcastle upon Tyne.
Following on from Gilly Fleming’s blog in November where she gave a fantastic update on some of the ways teaching can adapt to the challenges of the pandemic, we wanted to share with you our experience of developing a new learning tool and applying it in such an unusual time.
The challenges of working as a collaborative team, prototyping an idea, testing and trialing the model – all with minimal face-to-face contact – have certainly tested our patience and resolve. However, the results have been very encouraging and we have found it to be especially valuable during the current pandemic restrictions and adjustments. We can also see potential for more development and would be keen to hear from others who might be working on similar ideas.
A Random Patient Generator
We’ve faced a number of challenges over the last 12 months, similar to nearly everyone else in the country. Something we’ve found particularly difficult in the critical care environment is keeping training going; finding the time to make learning happen and keeping this open and accessible when nearly everything is locked down and behind some form of PPE is very hard. We have also seen a massive increase in video conferencing which has resulted in screen fatigue and created barriers to many traditional methods of teaching.
To help us address this, we consolidated a project we had been working on for a few months prior to the coronavirus situation – a random patient generator. To give you an idea of how this tool can help learning be a little less formal and much more accessible, here are a couple of the title ideas: “Jumanji: welcome to the ICU” and “The Randomiser”. What are we talking about? Let us explain.
A random patient generator is a way of rapidly constructing a hypothetical patient or scenario that can be used to facilitate teaching or discussion. It is not an entirely new concept – they have been used in a number of areas before but, in general, the implementations have been a little limited in scope. Having seen a random patient generator used in medical student teaching, we felt this could be used to stimulate learning for groups of differing knowledge, backgrounds and abilities, as well as groups at more similar levels such as core specialty trainees. It offered the advantage that by the very nature of a randomly generated scenario, there is no preparation required for a session and it also had the potential to bring a more informal and light-hearted atmosphere to tutorials, possibly even gamifying the learning. We spent some time researching how others have approached the process and then proceeded to develop and roll out the idea.
How does it work?
The random patient is produced from a database containing the key elements of a variety clinical scenarios. We have constructed the database such that these elements are separated into a base set that is required to “build” a patient or scenario (we have chosen: age, past medical history, location and acute or focus condition) and a set of additional more challenging variables which can be used to expand the scope or deepen the complexity of a scenario for more senior groups (physiological variables, surgical procedure, “complex” issues and emergency scenarios).
We tested and fine-tuned our database using hard copies (cards) which we could shuffle and thereby produce random selections. We have needed to check carefully to ensure that elements would not clash or repeat as this would be unhelpful and distracting. Once we had settled on our initial collection of variables, we changed to using an electronic format. This can be in the form of a report generated straight from the database or via animated selection “wheels”. These wheels help to break the ice at the beginning of sessions and have been affectionately called the Wheels of Misfortune.
The facilitator for the session will give a short announcement prior to generating the random patient. This outlines the aims and rules of the session, and sets the overall tone. Then the scenario is created either by dealing physical cards or by spinning our selection wheels. We have tended to begin the discussion by having the facilitator nominate a participant to describe their thoughts when initially seeing the scenario. This can be a way of helping a more junior or less confident member of group engage, particularly if they perceive they have little knowledge on a topic. Key elements of the facilitator’s role are to maintain a non-threatening atmosphere and to divert any tendencies to turn the tutorial into a didactic teaching session. However, the exploration of specific areas of knowledge and sharing of expertise, especially when written up on a whiteboard, has often had clear positive effects on groups.
At times during the dialogue, it may become apparent that the development of the themes may benefit from a partial re-randomisation. In this situation most of the scenario is maintained but one key element is changed – either by a choice of the facilitator or by repeating the random selection process. This may also allow comparing and contrasting segments of thought processes, decision making and cognitive biases. On other occasions, the case may not be suitably challenging for the group and then the facilitator can expand with the additional more challenging variables. By having this degree of flexibility, we have found the sessions can cater for any level of experience or knowledge.
At the end of each session, the facilitator summarises the learning points that they have observed and checks them with the rest of the participants. This has sometimes brought up different reflection points which can be enlightening for the facilitator as well as the rest of the group.
“I cannot teach anybody anything I can only make them think”
Socrates
The random patient generator sessions take their educational cues from a number of areas of learning theory: humanism, constructivism and relational understanding. The sessions are humanist in their emphasis on small group, comfortable, low pressure settings. The building of understanding through activating current knowledge of a subject and linking it to new details or information suggested by another member of the group fits within a constructivist framework. This aligns with SOLO taxonomy where we see the progression from unistructural knowledge through to multi-structural or relational understanding.
In keeping with the constructivist theme there is much emphasis on the session lead taking a facilitator role as opposed to a teacher role. This set up is almost mandated by the fact that the content of the session is unknown in advance and therefore requires minimal or no preparation time. The aim of a session is to facilitate and encourage dynamic self-learning, not to deliver a pre-prepared lesson full of facts and figures for the participants to soak up.
It is desirable for the facilitator to manage the environment so that discussion is generated within the group and freedom of speech is promoted. Interestingly, the facilitator can also participate as a learner and we encourage fostering the flat hierarchy. This allows exploration of ideas and the creation of a safe place for individuals to think and voice their thoughts and ideas. An exciting element of this approach is the ability to share tacit (or implicit) learning which is notoriously difficult.
Implementation
The feedback from those attending has been universally positive and many of the responses praised the sessions’ ability to enable interaction and participation quickly. This is particularly encouraging as most participants are using the random patient generator for the first time. Participants reported having rapidly engaged with the sessions and leaving with something to reflect on but, in most cases, having learnt something concrete as well.
At times it has proven so popular that it has been difficult to stop the sessions or ignore requests to generate another scenario. Comments have included quotes like “it is exciting that no-one knows what is coming next including the facilitator”, “it… made me feel as a participant like everyone was on the same level and at the same starting point, which encourages contribution and makes it feel less intimidating”. The lack of requirement for specific preparation was also felt to be beneficial as that can be a barrier to some formal teaching sessions.
Another aspect that has been interesting when exploring how these random scenarios might assist in learning is that a patient may be generated that does not fit into a “text-book” case. This has been highlighted by those attending as it allowed them to think beyond the classic presentations and approach scenarios that they felt were more like real life. This reflected how they needed to use and access knowledge in their working lives.
During our early tests we learned a number of points about facilitating the random patient generator sessions:
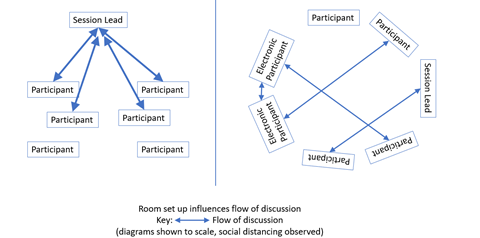
- Room set up/lay out can significantly impact the session facilitator’s role
Having the room laid out with a circle of chairs rather than all facing the front changes the focus away from the facilitator to the group as a whole. Interestingly, so long as microphone and video feeds are working appropriately, those attending electronically can be made to feel just as much a part of that circle of participants as those attending in person.
- Perceived level/grade of the facilitator relative to the group.
Although we have had success with consultants facilitating the sessions and being active participants, we have noticed that having a facilitator who is peer to the participants seems to trigger discussion which flows around the group rather than back and forth to the facilitator. It is perhaps understandable that this occurs when a consultant facilitates the session as the participants see this person as the lead and seek validation of their statements and opinions.
To help cement the facilitator role we have developed an introduction script which can be read at the beginning of the session to set the right atmosphere and outline the set up, aims and basic group rules. We hope that this script will allow the facilitator to be anyone from the group rather than the most senior participant or the participant with the most interest in teaching. We are also looking forward to trialling the session with the facilitator joining remotely via videoconferencing and we hope that this script will help to achieve this.
Where can this develop to?
We are hoping to develop the random patient generator over the coming months and below are a few areas we are planning to focus on.
Production of app-based content
So far the random patient generator has developed from a proof of concept as a physical deck of hand written address cards to a spreadsheet with a randomisation function and the ‘Wheel of Misfortune’ web-based selection wheels. Our plan is to maximise the portability and accessibility of the random patient generator further enabling its use for ad hoc/ or last minute sessions. To achieve this we are looking into the practicalities and finance of developing a mobile device optimised web page or app. This would allow loading up the app, clicking a button and producing a random patient. The electronic version potentially allows for further refinement of the randomiser with the addition of filters to adjust and curate the output for the participant group. Filters could add/remove advanced issues, focus on certain past medical histories or themes of emergencies. They could also better facilitate specialty or sub-specialty learning such as paediatrics or obstetric critical care.
Expansion to multidisciplinary groups
To date our sessions have been attended by medical and Advanced Critical Care Practitioner staff. As we all know ICM is a team game and we are very keen to trial the use of the random patient generator to facilitate multidisciplinary team (MDT) learning. We feel that the relaxed, open discussion format alongside the emphasis on group engagement should result in valuable sessions which help participants appreciate how the management and approach to a patient differs amongst the MDT. This process is hoped to foster learning from each other and bringing the MDT together with a deeper understanding of each other’s role.
Refining facilitator script
We will continue to refine the facilitator’s introduction script as it is clear from our pilot sessions that the wording of this script is important in setting the session off in a particular direction. The most valuable session direction can be achieved with relatively subtle changes to the introduction. Thinking beyond this is the potential to use the random patient generator to explore topics which are not often covered. Examples we are keen to explore are clinical decision making and cognitive bias. These tricky session topics would benefit from the small group, reflective, self-learning afforded by the random patient generator. An altered introduction script would aim to direct the group discussion through the appropriate lens but without sign-posting the learning points too clearly as that might undermine the value of the learning process and discussion.
We hope that you have enjoyed reading about our current project. If you have any previous experiences learning with or facilitating sessions using a random patient generator and you would like to share or discuss them, please don’t hesitate to contact us.